Inside Angle
From 3M Health Information Systems

The telemedicine wave: Good or bad?
Telemedicine has exploded during the COVID-19 pandemic with expanded access guidelines from the CDC and others.[1] How much of this is a good thing? Should we continue the new rules as the new norm, or should we go back to the old rules when the pandemic finally wanes? One reads and hears of positive anecdotes.
The boom in telephone and video visits has led to a boom in recommendations on how to bill for these encounters [2] and one might wonder if this new stream of spending will result in more than just increased costs.
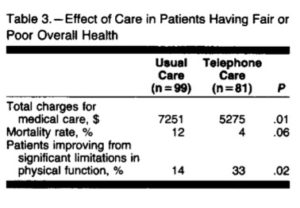
There has been good evidence on the benefits of allowing telephone and video interactions. In a randomized trial published in 1992, John Wasson et al found that patients in the “telephone care” arm had lower costs, lower mortality and improved physical function (Table 3 below).[3]
I was on a call recently with a number of chief medical officers of insurance plans. Representatives of companies in the telemedicine business described very positive responses from patients and providers with this mode of care. A telephone visit with or without video can meet many needs, reserving face-to-face visits for times when that is the best option.
Ultimately, how will we know if the policies should remain open or go back? The decision should be driven by data. Telemedicine impacts the satisfaction with care received (patient experience), with care delivered (provider satisfaction) and, if done well may as Wasson demonstrated, actually improves access to care and thus reduces potentially preventable downstream events (potentially preventable office visits, emergency room visits, hospitalizations, hospital readmissions for instance). If done well, we might expect – as in Wasson’s study – that expanded access to telephone and video care results in reduced total cost of care.
As the televisit claims roll in, it is important to take the time to analyze the impact. I suspect that we will see a range of outcomes – some will do this well, others maybe not so well. We’ll see the differences in the data and can adjust policy and programs accordingly.
L. Gordon Moore, MD, is senior medical director, Clinical Strategy and Value-based Care for 3M Health Information Systems.
More time with patients, less time with technology. That’s creating time to care.
[1] https://www.cdc.gov/coronavirus/2019-ncov/hcp/telehealth.html Accessed 7/6/20
[2] https://www.acponline.org/practice-resources/covid-19-practice-management-resources/telehealth-coding-and-billing-during-covid-19 Accessed 7/6/20
[3] https://pubmed.ncbi.nlm.nih.gov/1545464/ Accessed 7/6/20


L. Gordon Moore, MD
Former Senior Medical Director, Clinical Strategy and Value-based Care
L Gordon Moore, MD, is the former senior medical director of clinical strategy and value-based care for 3M Health Information Systems. In this role he bridges the intersections of quality,…