Inside Angle
From 3M Health Information Systems

Are we being more specific?
One of the main drivers for moving to ICD-10 was increased coding specificity. When the switch took place, however, it was acknowledged that it might still take some time for clinical documentation to support the increased specificity of the new coding system. CMS allowed a one-year grace period on reimbursement impacts due to the use of unspecified codes. With the expiration of that grace period last October, we’ve started to explore shifts in the specificity of codes being used. For this month’s post, I thought it would be interesting to show one example where the changes are becoming noticeable: Atrial Fibrillation.
For purposes of this example, I’m going to look at inpatient visits with codes that deal with the single condition of Atrial Fibrillation (irregular heartbeat). These are:
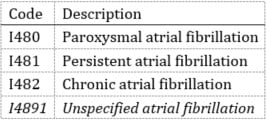
I’m not considering visits that were coded with combination codes such as:

So let’s start by looking at October 2015 data from more than 1,000 3M client facilities following the implementation of ICD-10. For that month, here’s what the data looks like:
- 97,676 – Total Inpatient visits with one of the 4 codes above.
- 52,518 – Visits coded with a specified code (I480, I481, I482)
- 45,158 – Visits coded with the unspecified code of I4891
That means that 46.2 percent of visits in our baseline group were coded with the unspecified code.
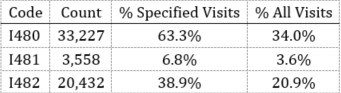
Let’s look a little closer at the distribution of those 52,518 visits that were specific. They break down like this:
Okay, so that’s where we started in October of 2015. Now, let’s see what it looks like over a year later in January 2017. In this set of data we have:
- 160,083 – Total Inpatient visits with one of the 4 codes above.
- 97,996 – Visits coded with a specified code (I480, I481, I482)
- 62,087 – Visits coded with the unspecified code of I4891
That means that only 38.8 percent of visits in the comparison group were coded with the unspecified code. Note that this is more than a seven percent decrease in visits coded with the unspecified code.
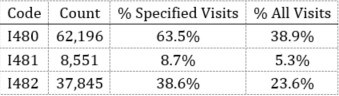
This is how the 97,996 visits that were specifically coded in January 2017 break down:
This one example is promising. Not only is there a shift from seven percent unspecified codes towards more specific codes, but the data also indicates that those visits were not spread evenly across the three different specific codes. The second data set is larger than the first, but both are large enough for this difference to be significant. This raises interesting questions about why one specific code might rise more than another:
- Is there actually higher incidence of one type of Atrial Fibrillation than another?
- Have documentation improvement efforts to date simply been more successful in one area than another?
- Would we see similar results with another condition such as Congestive Heart Failure?
- How much variation is there in these changes between different enterprises?
- How much might the continued use of unspecified codes affect reimbursement?
- Are there differences in how individual coders are handling specificity?
These are some of the types of questions we’ll be investigating in the coming months. Stay tuned!
Jason Mark is a business intelligence architect, Emerging Business Technology with 3M Health Information Systems.


Jason Mark
Manager
Jason Mark is manager, Research & Applied Data Science Lab for 3M Health Information Systems, Inc. Jason has been with 3M HIS since 2005. Prior to his current position, Jason…